Scabies (from Latin: scabere, "to scratch"), known colloquially as the seven-year itch, is a contagious skin infection that occurs among humans and other animals. It is caused by a tiny and usually not directly visible parasite, the mite Sarcoptes scabiei, which burrows under the host's skin, causing intense allergic itching. The infection in animals (caused by different but related mite species) is called sarcoptic mange.
The disease may be transmitted from objects but is most often transmitted by direct skin-to-skin contact, with a higher risk with prolonged contact. Initial infections require four to six weeks to become symptomatic. Reinfection, however, may manifest symptoms within as little as 24 hours. Because the symptoms are allergic, their delay in onset is often mirrored by a significant delay in relief after the parasites have been eradicated. Crusted scabies, formerly known as Norwegian scabies, is a more severe form of the infection often associated with immunosuppression.
The disease can be effectively treated with a number of medications. Permethrin cream is the most effective, but expensive compared to other treatments.Crotamiton is less effective, but also nontoxic and soothing. Ivermectin may be used orally and topically. Treatment with lindane preparations has fallen out of favor due to high toxicity and parasite resistance. In order to prevent re-infection, the host's contacts are also often treated
Signs and symptoms
The characteristic symptoms of a scabies infection include intense itching and superficial burrows. The burrow tracks are often linear, to the point that a neat "line" of four or more closely placed and equally developed mosquito-like "bites," is almost diagnostic of the disease.
Pathophysiology
The symptoms are caused by an allergic reaction of the host's body to mite proteins, though exactly which proteins remains a topic of study. The mite proteins are also present from the gut, in mite feces, which are deposited under the skin. The allergic reaction is both of the delayed (cell-mediated) and immediate (antibody-mediated) type, and involves IgE (antibodies, it is presumed, mediate the very rapid symptoms on re-infection). The allergy-type symptoms (itching) continue for some days, and even several weeks, after all mites are killed. New lesions may appear for a few days after mites are eradicated. Nodular lesions from scabies may continue to be symptomatic for weeks after the mites have been killed.


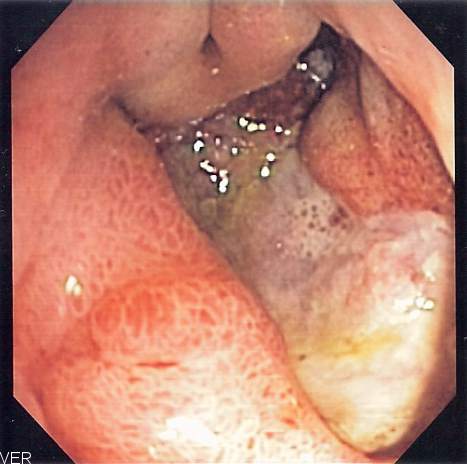
A peptic ulcer, also known as PUD or peptic ulcer disease, the most common ulcer of an area of the gastrointestinal tract that is usually acidic and thus extremely painful. It is defined as mucosal erosions equal to or greater than 0.5 cm. As many as 70–90% of such ulcers are associated withHelicobacter pylori, a spiral-shaped bacterium that lives in the acidic environment of the stomach; however, only 40% of those cases go to a doctor. Ulcers can also be caused or worsened by drugs such as aspirin, Plavix (clopidogrel), ibuprofen, and other NSAIDs.
Signs and symptoms
- abdominal pain, classically epigastric with severity relating to mealtimes, after around three hours of taking a meal (duodenal ulcers are classically relieved by food, while gastric ulcers are exacerbated by it);
- bloating and abdominal fullness;
- waterbrash (rush of saliva after an episode of regurgitation to dilute the acid in esophagus - although this is more associated with GERD);
- nausea, and copious vomiting;
- loss of appetite and weight loss;
- hematemesis (vomiting of blood); this can occur due to bleeding directly from a gastric ulcer, or from damage to the esophagus from severe/continuing vomiting.
- melena (tarry, foul-smelling feces due to oxidized iron from hemoglobin);
- rarely, an ulcer can lead to a gastric or duodenal perforation, which leads to acute peritonitis. This is extremely painful and requires immediate surgery.
A history of heartburn, gastroesophageal reflux disease (GERD) and use of certain forms of medication can raise the suspicion for peptic ulcer. Medicines associated with peptic ulcer include NSAID (non-steroid anti-inflammatory drugs) that inhibit cyclooxygenase, and most glucocorticoids (e.g. dexamethasone and prednisolone).
In patients over 45 with more than two weeks of the above symptoms, the odds for peptic ulceration are high enough to warrant rapid investigation by EGD (see below).
The timing of the symptoms in relation to the meal may differentiate between gastric and duodenal ulcers: A gastric ulcer would give epigastric pain during the meal, as gastric acid production is increased as food enters the stomach. Symptoms of duodenal ulcers would initially be relieved by a meal, as the pyloric sphincter closes to concentrate the stomach contents, therefore acid is not reaching the duodenum. Duodenal ulcer pain would manifest mostly 2–3 hours after the meal, when the stomach begins to release digested food and acid into the duodenum.
Also, the symptoms of peptic ulcers may vary with the location of the ulcer and the patient's age. Furthermore, typical ulcers tend to heal and recur and as a result the pain may occur for few days and weeks and then wane or disappear. Usually, children and the elderly do not develop any symptoms unless complications have arisen.
Burning or gnawing feeling in the stomach area lasting between 30 minutes and 3 hours commonly accompanies ulcers. This pain can be misinterpreted as hunger, indigestion or heartburn. Pain is usually caused by the ulcer but it may be aggravated by the stomach acid when it comes into contact with the ulcerated area. The pain caused by peptic ulcers can be felt anywhere from the navel up to the sternum, it may last from few minutes to several hours and it may be worse when the stomach is empty. Also, sometimes the pain may flare at night and it can commonly be temporarily relieved by eating foods that buffer stomach acid or by taking anti-acid medication. However, peptic ulcer disease symptoms may be different for every sufferer.
Treatment
Younger patients with ulcer-like symptoms are often treated with antacids or H2 antagonists before EGD is undertaken. Bismuth compounds may actually reduce or even clear organisms though the warning labels of some bismuth subsalicylate products indicate that the product should not be used by someone with an ulcer.
Patients who are taking nonsteroidal anti-inflammatories (NSAIDs) may also be prescribed a prostaglandin analogue (Misoprostol) in order to help prevent peptic ulcers, which may be a side-effect of the NSAIDs.
When H. pylori infection is present, the most effective treatments are combinations of 2 antibiotics (e.g. Clarithromycin, Amoxicillin, Tetracycline, Metronidazole) and 1 proton pump inhibitor (PPI), sometimes together with a bismuth compound. In complicated, treatment-resistant cases, 3 antibiotics (e.g. amoxicillin + clarithromycin + metronidazole) may be used together with a PPI and sometimes with bismuth compound. An effective first-line therapy for uncomplicated cases would be Amoxicillin + Metronidazole + Pantoprazole (a PPI). In the absence of H. pylori, long-term higher dose PPIs are often used.
Treatment of H. pylori usually leads to clearing of infection, relief of symptoms and eventual healing of ulcers. Recurrence of infection can occur and retreatment may be required, if necessary with other antibiotics. Since the widespread use of PPI's in the 1990s, surgical procedures (like "highly selective vagotomy") for uncomplicated peptic ulcers became obsolete.
Perforated peptic ulcer is a surgical emergency and requires surgical repair of the perforation. Most bleeding ulcers require endoscopy urgently to stop bleeding with cautery, injection, or clipping.
Ranitidine provides relief of peptic ulcers, heartburn, indigestion and excess stomach acid and prevention of these symptoms associated with excessive consumption of food and drink. Ranitidine is available over the counter from a pharmacy and works by decreasing the amount of acid the stomach produces allowing healing of ulcers. Zantac tablets contain Ranitidine 150 mg as the active ingredient which can also be bought generically.
Sucralfate, (Carafate) has also been a successful treatment of peptic ulcers.
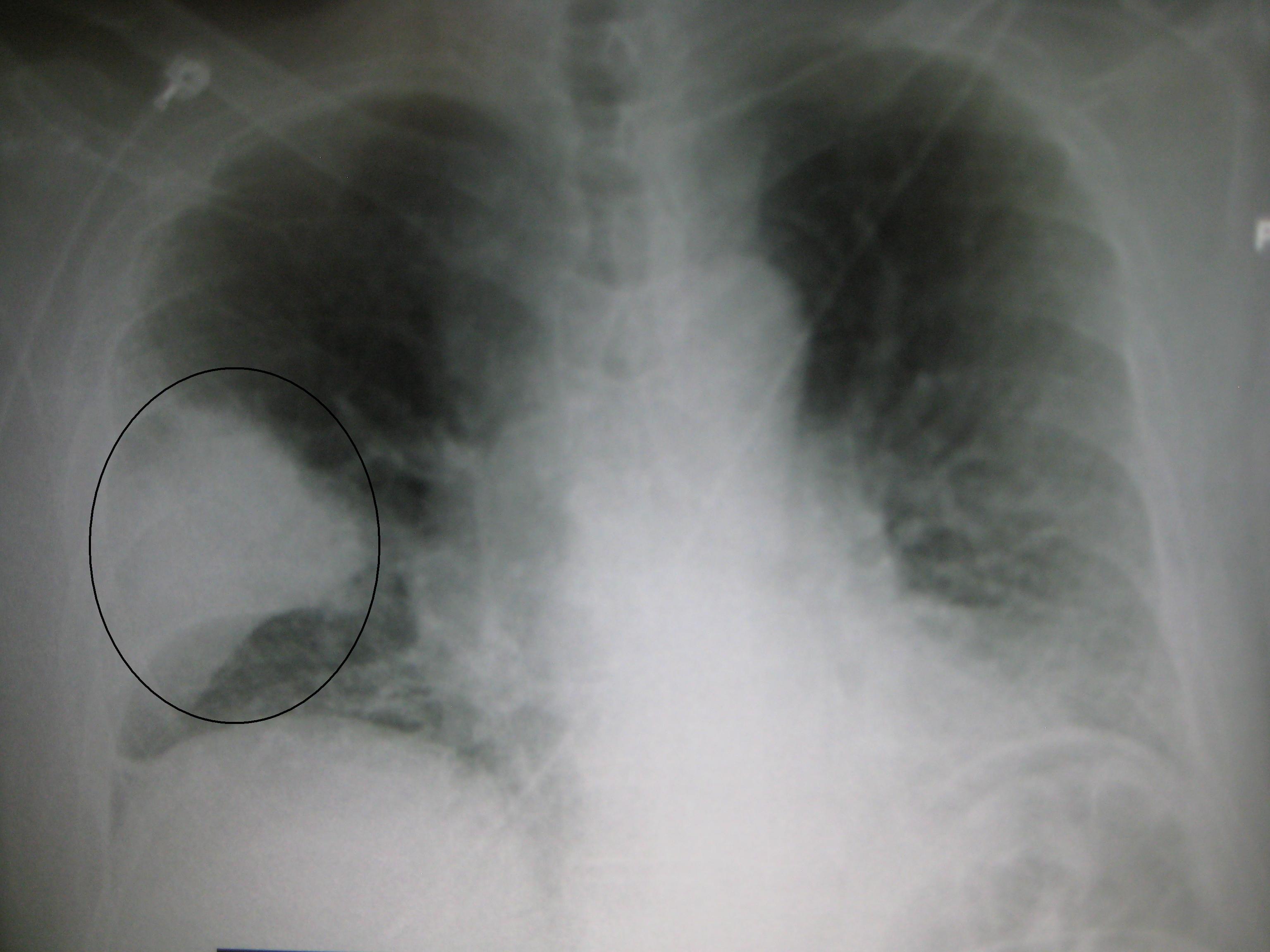
Colles' fracture
A Colles' fracture, also Colles fracture, is a fracture of the distal radius in the forearm with dorsal (posterior) displacement of the wrist and hand. The fracture is sometimes referred to as a "dinner fork" or "bayonet" deformity due to the shape of the resultant forearm. For a more detailed discussion seedistal radius fracture.
Causes
The fracture is most commonly caused by people falling onto a hard surface and breaking their fall with outstretched arms - falling with wrists flexed would lead to a Smith's fracture. It can also be caused by overuse. Orignally it was described in elderly people, post-menopausal women. It usually occurs about an inch or two proximal to the radio-carpal joint with posterior and lateral displacement of the distal fragment resulting in the characteristic "dinner fork" or "bayonet" like deformity.Colles' fracture is a common fracture in people with osteoporosis, second only to vertebral fractures.
Treatment
Management depends on the severity of the fracture. An undisplaced fracture may be treated with a cast alone.The cast is applied with the distal fragment inpalmar flexion and ulnar deviation. A fracture with mild angulation and displacement may require closed reduction. There is some evidence that immobilization with the wrist in dorsiflexion as opposed to palmarflexion results in less redisplacement and better functional status. Significant angulation and deformity may require an open reduction and internal fixation or external fixation. The volar forearm splint is best for temporary immobilization of forearm, wrist and hand fractures, including Colles' fracture There are several established instability criteria: dorsal tilt >20°, comminuted fracture, abruption of the ulnar styloid process, intraarticular displacement >1mm, loss of radial height >2mm.A higher amount of instability criteria increases the likelihood of operative treatment.Treatment modalities differ in the elderly.

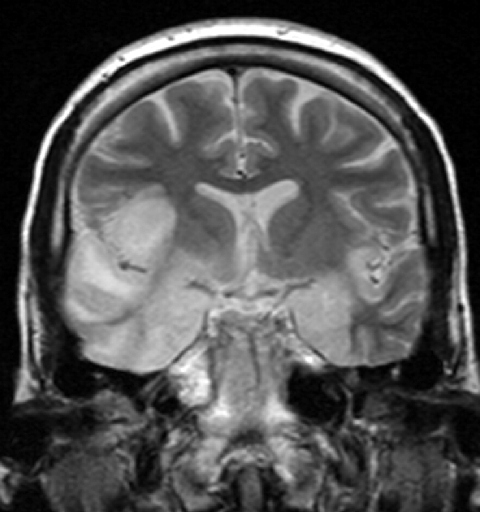
Myxedema
Myxedema (British English: myxoedema) describes a specific form of cutaneous and dermal edema secondary to increased deposition of connective tissuecomponents (like glycosaminoglycans, hyaluronic acid, and other mucopolysaccharides) in subcutaneous tissue as seen in various forms of hypothyroidismand Graves' disease.]:535 It is more common in women than in men. Cause
The increased deposition of glycosaminoglycan is not fully understood, however two mechanisms predominate.
- Exophthalmos in particular results from TSH receptor stimulation on fibroblasts behind the eyes which leads to increased glycosaminoglycan deposition. It is thought that many cells responsible for forming connective tissue react to increases in TSH levels.
- Secondarily, in autoimmune thyroid diseases lymphocytes react to the TSH receptor. Thus, in addition to the inflammation within the thyroid, any cell that expresses the TSH receptor will likely experience lymphocytic infiltrates as well. The inflammation can cause tissue damage and scar tissue formation, explaining the deposition of glycosaminoglycans.The increased deposition of glycosaminoglycans causes an osmotic edema and fluid collection.Hashimoto's thyroiditis is the most common cause of myxedema in the United States.
Symptoms
Symptoms of myxedema include thickening of the skin and other symptoms associated with hypothyroidism, including fatigue, weight gain, Depression, dry skin, and brittle hair, among others. Skin thickening or swelling associated with myxedema is often described as nonpitting edema. In other words, if you press on the skin of the affected area and then remove your finger, you will not see an imprint.
TREATMENTS
Myxedema is most often addressed by treating the underlying cause of hypothyroidism that led to the thickening and coarseness of the skin. Medication to replace the reduced thyroid hormones is the most common treatment, and when dosed appropriately, may halt the progression of myxedem