Leptospirosis
Leptospirosis (also known as Weil's syndrome, canicola fever, canefield fever, nanukayami fever, 7-day fever, Rat Catcher's Yellows, Fort Bragg fever, black jaundice and Pretibial fever:290) is caused by infection with bacteria of the genus Leptospira, and affects humans as well as other mammals, birds, amphibians, and reptiles.
The disease was first described by Adolf Weil in 1886 when he reported an "acute infectious disease with enlargement of spleen, jaundice and nephritis". Leptospira was first observed in 1907 from a post mortem renal tissue slice. In 1908, Inada and Ito first identified it as the causative organism and in 1916 noted its presence in rats.
Though recognised among the world's most common diseases transmitted to people from animals, leptospirosis is nonetheless a relatively rare bacterial infection in humans. The infection is commonly transmitted to humans by allowing water that has been contaminated by animal urine to come in contact with unhealed breaks in the skin, the eyes, or with the mucous membranes. Outside of tropical areas, leptospirosis cases have a relatively distinct seasonality with most of them occurring in spring and autumn.
1 Causes
2 Symptoms
3 Complications
4 Diagnosis
5 Prevention and treatment
6 Epidemiology
7 History
8 References
9 Further reading
10 External links
Scanning electron micrograph of a number of Leptospira sp. bacteria atop a 0.1 µm polycarbonate filter
Leptospirosis is caused by a spirochaete bacterium called Leptospira spp. There are at least five serovars of importance in the United States and Canada, all of which cause disease in dogs (Icterohaemorrhagiae, Canicola, Pomona, Grippotyphosa, and Bratislava).
There are other (less common) infectious strains. Genetically different leptospira organisms may be identical serologically and vice versa. Hence, an argument exists on the basis of strain identification. The traditional serologic system is seemingly more useful from a diagnostic and epidemiologic standpoint at the moment (which may change with further development and spread of technologies like polymerase chain reaction (PCR)).
Leptospirosis is transmitted by the urine of an infected animal and is contagious as long as it is still moist. Although rats, mice and moles are important primary hosts, a wide range of other mammals including dogs, deer, rabbits, hedgehogs, cows, sheep, raccoons, opossums, skunks, and certain marine mammals are able to carry and transmit the disease as secondary hosts. Dogs may lick the urine of an infected animal off the grass or soil, or drink from an infected puddle. There have been reports of "house dogs" contracting leptospirosis apparently from licking the urine of infected mice that entered the house. The type of habitats most likely to carry infective bacteria are muddy riverbanks, ditches, gullies, and muddy livestock rearing areas where there is regular passage of either wild or farm mammals. There is a direct correlation between the amount of rainfall and the incidence of leptospirosis, making it seasonal in temperate climates and year-round in tropical climates.
Leptospirosis is also transmitted by the semen of infected animals Slaughterhouse workers may contract the disease through contact with infected blood or body fluids.
Humans become infected through contact with water, food, or soil containing urine from these infected animals. This may happen by swallowing contaminated food or water, or through skin contact. The disease is not known to be spread from person to person and cases of bacterial dissemination in convalescence are extremely rare in humans. Leptospirosis is common among water-sport enthusiasts in specific areas as prolonged immersion in water is known to promote the entry of the bacteria. Surfers and whitewater paddlers are at especially high risk in areas that have been shown to contain the bacteria, and can contract the disease by swallowing contaminated water, splashing contaminated water into their eyes or nose, or exposing open wounds to infected water.] Occupations at risk include veterinarians, slaughterhouse workers, farmers, sewer workers, and people working on derelict buildings. Rowers are also sometimes known to contract the disease.
[edit]Symptoms
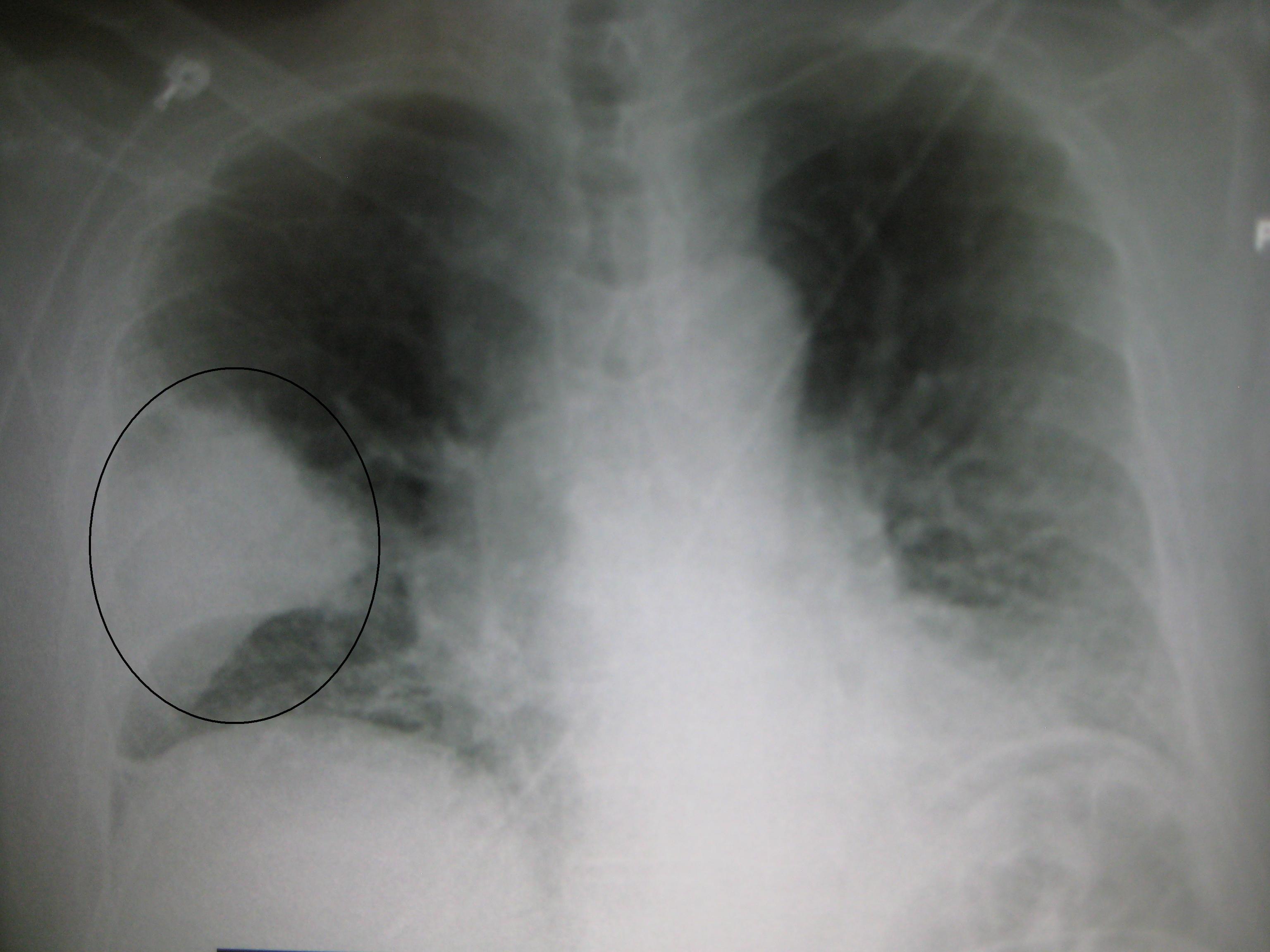
Leptospiral infection in humans causes a range of symptoms, and some infected persons may have no symptoms at all. Leptospirosis is a biphasic disease that begins with flu-like symptoms (fever, chills, myalgias, intense headache). The first phase resolves, and the patient is briefly asymptomatic until the second phase begins. This is characterized by meningitis, liver damage (causing jaundice), and renal failure. The infection is often wrongly diagnosed due to the wide range of symptoms. This leads to a lower registered number of cases than exists. Symptoms of leptospirosis include high fever, severe headache, chills, muscle aches, and vomiting, and may include jaundice, red eyes, abdominal pain, diarrhea, and rash. Initial presentation may resemble pneumonia. The symptoms in humans appear after a 4–14 day incubation period.
The incubation period (time of exposure to first symptoms) in animals is anywhere from 2 to 20 days. In dogs the liver and kidney are most commonly damaged by leptospirosis. In addition, there are recent reports of a pulmonary form of canine leptospirosis associated with severe hemorrhage in the lungs similar to the human pulmonary hemorrhagic syndrome.Vasculitis may occur, causing edema and potentially disseminated intravascular coagulation (DIC). Myocarditis, pericarditis, meningitis, and uveitis are also possible sequelae.[5] One should strongly suspect leptospirosis and include it as part of a differential diagnosis if the sclerae of the dog's eyes appear jaundiced (even slightly yellow). The absence of jaundice does not eliminate the possibility of leptospirosis, and its presence could indicate hepatitis or other liver pathology rather than leptospirosis. Vomiting, fever, failure to eat, reduced urine output, unusually dark or brown urine, and lethargy are also indications of the disease.
[edit]Complications
Complications include meningitis, extreme fatigue, hearing loss, respiratory distress, azotemia, and renal interstitial tubular necrosis, which results in renal failure and often liver failure (the severe form of this disease is known as Weil's disease, though it is sometimes named Weil Syndrome). Cardiovascular problems are also possible.
[edit]Diagnosis
Kidney tissue, using a silver staining technique, revealing the presence of Leptospira bacteria
On infection the microorganism can be found in blood for the first 7 to 10 days (invoking serologically identifiable reactions) and then moving to the kidneys. After 7 to 10 days the microorganism can be found in fresh urine. Hence, early diagnostic efforts include testing a serum or blood sample serologically with a panel of different strains. It is also possible to culture the microorganism from blood, serum, fresh urine and possibly fresh kidney biopsy. Kidney function tests (Blood Urea Nitrogen and creatinine) as well as blood tests for liver functions are performed. The latter reveal a moderate elevation of transaminases. Brief elevations of aspartate aminotransferase (AST), alanine aminotransferase (ALT), and gamma-glutamyltransferase (GGT) levels are relatively mild. These levels may be normal, even in children with jaundice. Diagnosis of leptospirosis is confirmed with tests such as Enzyme-Linked Immunosorbent Assay (ELISA) and polymerase chain reaction (PCR). Serological testing, the MAT (microscopic agglutination test), is considered the gold standard in diagnosing leptospirosis. As a large panel of different leptospira need to be subcultured frequently, which is both laborious and expensive, it is underused, mainly in developing countries.
Differential diagnosis list for leptospirosis is very large due to diverse symptomatics. For forms with middle to high severity, the list includes dengue fever and other hemorrhagic fevers, hepatitis of various etiologies, viral meningitis, malaria, and typhoid fever. Light forms should be distinguished from influenza and other related viral diseases. Specific tests are a must for proper diagnosis of leptospirosis. Under circumstances of limited access (e.g., developing countries) to specific diagnostic means, close attention must be paid to anamnesis of the patient. Factors such as certain dwelling areas, seasonality, contact with stagnant contaminated water (bathing swimming, working on flooded meadows, etc.) or rodents in the medical history support the leptospirosis hypothesis and serve as indications for specific tests (if available).
Leptospira can be cultured in Ellinghausen-McCullough-Johnson-Harris medium, which is incubated at 28 to 30 °C.[14] The median time to positivity is three weeks with a maximum of three months. This makes culture techniques useless for diagnostic purposes, but is commonly used in research.
[edit]Prevention and treatment
Doxycycline may be used as a prophylaxis 200–250 mg once a week, to prevent infection in adventure travelers to high risk areas.Treatment is a relatively complicated process comprising two main components: suppressing the causative agent and fighting possible complications. Aetiotropic drugs are antibiotics, such as cefotaxime, doxycycline, penicillin, ampicillin, and amoxicillin.
There are no human vaccines; animal vaccines are only for a few strains, and are only effective for a few months. Human therapeutic dosage of drugs is as follows: doxycycline 100 mg orally every 12 hours for 1 week or penicillin 1–1.5 MU every 4 hours for 1 week. In dogs, penicillin is most commonly used to end the leptospiremic phase (infection of the blood), and doxycycline is used to eliminate the carrier state.
Supportive therapy measures (especially in severe cases) include detoxification and normalization of the hydro-electrolytic balance. Glucose and salt solution infusions may be administered; dialysis is used in serious cases. Elevations of serum potassium are common and if the potassium level gets too high special measures must be taken. Serum phosphorus levels may likewise increase to unacceptable levels due to renal failure. Treatment for hyperphosphatemia consists of treating the underlying disease, dialysis where appropriate, or oral administration of calcium carbonate, but not without first checking the serum calcium levels (these two levels are related). Corticosteroids administration in gradually reduced doses (e.g., prednisolone starting from 30–60 mg) during 7–10 days is recommended by some[citation needed] specialists in cases of severe haemorrhagic effects. Organ specific care and treatment are essential in cases of renal, liver, or heart involvement.
[edit]Epidemiology
Annual rates of infection vary from 0.02 per 100,000 in temperate climates to 10 to 100 per 100,000 in tropical climates.
Nepal is experiencing a leptospirosis outbreak as of August 2010,[16] having favorable conditions like warm temperatures and moist soils. Cases increase in summer months (monsoon), but no accurate case count has been made as most go unreported.Almost all the higher animals and rodent hosts of Leptospira occur in Nepal.
[edit]History
The Native American lifestyle exposed them to the leptospiral life cycle.
Leptospirosis was postulated as the cause of an epidemic among Native Americans along the coast of present-day Massachusetts that occurred immediately before the arrival of the Pilgrims in 1620 and killed most of the native population.[18] Earlier proposals included plague, yellow fever, smallpox, influenza, chickenpox, typhus, typhoid fever, trichinellosis, meningitis, and syndemic infection of hepatitis B virus with the delta agent.None are as consistent with all the evidence as leptospirosis. While the disease may have been brought to the New World by Europeans, its spread was also influenced by the high-risk daily activities of the Native Americans. The leptospirosis hypothesis is supported by the occurrence of modern outbreaks identified as severe leptospirosis, some accompanied by high mortality rates (the Andaman Islands in the late 1980s, the Philippines in 2009, Ireland in 2010).
The cause of this epidemic has been a mystery, while other outbreaks in the same time frame are fairly well established. The epidemic is considered a pivotal event in American history since the failure of the Plymouth Colony might have meant the failure of British colonization in North America. A noted historian has said that the epidemic was the most important event in American history between the discovery of America by Columbus and the signing of the Declaration of Independence.[citation needed]
Before Weil's characterization in 1886, the disease known as infectious jaundice was very likely the same as Weil's disease, or severe icteric leptospirosis. During the Egyptian campaign, Napoleon's army suffered from what was probably infectious jaundice. Infectious jaundice occurred among troops during the American Civil War. It was also reported among troops at Gallipoli and other battles of World War I, where the sodden conditions of trench warfare favored infection. Terms used in early 20th century descriptions of leptospirosis include the pseudo-dengue of Java, seven-day fever, autumn fever, Akiyama disease, and marsh or swamp fever. L icterohaemorrhagieae was identified as the causative agent in pre-World War II outbreaks in Japan, which were characterized by jaundice and a high mortality rate.
In October 2010 British rower Andy Holmes died after contracting Weil's Disease.
In January 2011, Dr. Drew Pinsky, (Loveline, Celebrity Rehab) believes that he contracted leptospirosis while on vacation with his wife in the West Indies due to an outbreak at the time of their visit.
In July 2011 a Danish man died after contracting the disease, probably while cleaning up in his cellar after severe flooding. Heavy rainfall caused the sewers to overflow, flooding large areas of the Danish capital and killing approximately half the rats. The contaminated water got into many of cellars and overflowed into the streets, causing many people to come into contact with sewer water.
Leptospirosis
What is leptospirosis?
What are leptospirosis symptoms and signs?
How is leptospirosis diagnosed?
What is the treatment for leptospirosis? What is the prognosis for leptospirosis?
Can leptospirosis be prevented with a vaccine?
Can my pets get leptospirosis?
Leptospirosis At A Glance
Leptospirosis in Dogs
What are the signs of leptospirosis in pets?
The clinical signs of leptospirosis vary and are nonspecific. Sometimes pets do not have any symptoms. Common clinical signs reported in dogs include fever, vomiting, abdominal pain, diarrhea, refusal to eat, severe weakness and depression, stiffness, severe muscle pain, or inability to have puppies. Generally younger animals are more seriously affected than older animals.
SOURCE:
U.S. Centers for Disease Control and Prevention
What is leptospirosis?
Leptospirosis is an infectious disease caused by a type of bacteria called a spirochete. Leptospirosis can be transmitted by many animals such as rats, skunks, opossums, raccoons, foxes, and other vermin. It is transmitted though contact with infected soil or water. The soil or water is contaminated with the waste products of an infected animal. People contract the disease by either ingesting contaminated food or water or by broken skin and mucous membrane (eyes, nose, sinuses, mouth) contact with the contaminated water or soil.
Leptospirosis occurs worldwide, but it is most commonly acquired in the tropics. The U.S. Centers for Disease Control and Prevention states 100-200 cases of leptospirosis are reported each year in the United States, with about 50% of cases occurring in Hawaii. Although the incidence in the United States is relatively low, leptospirosis is considered the most widespread disease that is transmitted by animals in the world.
A 2010 outbreak in Michigan caused serious illness in numerous pets, raising concern for the local human population. In 2009, typhoons hit the Philippines, causing a leptospirosis outbreak. The Philippines Department of Health then reported 1,887 cases of leptospirosis, which resulted in 138 deaths.
What are leptospirosis symptoms and signs?
Leptospirosis symptoms begin from two to 25 days after initial direct exposure to the urine or tissue of an infected animal. This can even occur via contaminated soil or water. Veterinarians, pet shop owners, sewage workers, and farm employees are at particularly high risk. People participating in outdoor sporting activities like canoeing, rafting, hiking, and camping can also come into contact with contaminated water or soil.
The illness typically progresses through two phases:
The first phase of nonspecific flu-like symptoms includes headaches, muscle aches, eye pain with bright lights, followed by chills and fever. Watering and redness of the eyes occurs and symptoms seem to improve by the fifth to ninth day.
The second phase begins after a few days of feeling well. The initial symptoms recur with fever and aching with stiffness of the neck. Some patients develop serious inflammation of the nerves to the eyes, brain, spinal column (meningitis), or other nerves. Right upper area abdominal pain may occur. Less common symptoms relate to disease of the liver, lungs, kidneys, and heart.
Leptospirosis associated with liver and kidney disease is called Weil's syndrome and is characterized by yellowing of the eyes (jaundice). Patients with Weil's syndrome can also develop kidney disease and have more serious involvement of the organs affected.
Stroke
A stroke is occurs due to lack of blood to the brain which have a strong arm and thigh.
Thyroid
Thyroid is the thyroid gland growth only but the other parts of the thyroid gland looks normal which has arthritis and muscle pain.
Alcoholism
Alcoholism is chronic disease which has want to drink alcohol all time if not have alcohol will be like resist drug action.
Tuberculosis
Tuberculosis is caused by an infection caused by various strains of bacteria which Symptoms include chest pain, chills and night sweats.
coronary artery disease
A stroke is occurs due to lack of blood to the brain which have a strong arm and thigh.
Thyroid
Thyroid is the thyroid gland growth only but the other parts of the thyroid gland looks normal which has arthritis and muscle pain.
Alcoholism
Alcoholism is chronic disease which has want to drink alcohol all time if not have alcohol will be like resist drug action.
Tuberculosis
Tuberculosis is caused by an infection caused by various strains of bacteria which Symptoms include chest pain, chills and night sweats.
coronary artery disease
The flow of blood to the heart causes ischemia of the heart muscle cells which associated with smoking, diabetes and high blood pressure.
Definition type
เป็นชนิดของสิ่งแนะที่ชี้แสดงความหมายหรือนิยามคำศัพท์ที่ไม่คุ้นเคย
ซึ่งผู้อ่านสามารถสังเกตการนิยามความหมายของคำศัพท์ได้โดยการดูที่ตัวชี้แนะ หรือคำสัญญาณ
(clues signal words) ที่ปรากฏอยู่ในข้อความนั้นๆ ตัวชี้แนะหรือคำสัญญาณ ได้แก่
verb "to be" be called
mean(s/ed) called
consist of may be seen as
refer to can be defined as
may be described as can be taught of
what this means is
คำชี้แนะหรือคำสัญญาณดังกล่าวมาข้างต้นนี้ มีความหมายในทำนองเดียวกัน นั่นคือ
แปลว่า "คือ , หมายถึง , หมายความว่า, เรียกว่า"
ตัวอย่าง- A premise is a statement of the relationship between a cause and a consequence.
อธิบาย premise เป็นคำศัพท์ที่ไม่คุ้นเคยis เป็นคำชี้แนะ หรือคำสัญญาณa statement of the relationship เป็นคำนิยามหรือความหมายของคำว่า premiseดังนั้น premise ก็คือ ข้อความที่แสดงความสัมพันธ์ระหว่างสาเหตุและผลลัพธ์- People who study the stars are called astronomers.
อธิบาย astronomers เป็นคำศัพท์ที่ไม่คุ้นเคยare called เป็นคำชี้แนะหรือคำสัญญาณpeople who study the stars เป็นคำนิยามหรือความหมายของคำว่า astronomersดังนั้น astronomers ก็คือ
คนที่ศึกษาเรื่องดวงดาว หรือนักดาราศาสตร์ นั่นเอง- A committee may be defined as any group interacting in regard to a common purpose.
อธิบาย committee เป็นคำที่ไม่คุ้นเคยmay be defined as เป็นคำสัญญาณ หรือตัวชี้แนะany group interacting in reagard to common purpose เป็นคำนิยามหรือความหมายของคำว่า committee ดังนั้น committee ก็คือ กลุ่ม หรือคณะบุคคลที่กระทำการใดๆ โดยมีจุดประสงค์ร่วมกัน
Pneumonia
Main article: Classification of pneumonia
Pneumonitis refers to lung inflammation; pneumonia refers to pneumonitis, usually due to infection but sometimes non infectious, that has the additional feature of pulmonary consolidation.Pneumonia can be classified in several ways. It is most commonly classified by where or how it was acquired (community-acquired, aspiration, healthcare-associated, hospital-acquired, and ventilator-associated pneumonia),but may also be classified by the area of lung affected (lobar pneumonia, bronchial pneumonia and acute interstitial pneumonia),or by the causative organism.Pneumonia in children may additionally be classified based on signs and symptoms as non-severe, severe, or very severe.
Signs and symptoms.
Main symptoms of infectious pneumonia
People with infectious pneumonia often have a productive cough, fever accompanied by shaking chills, shortness of breath, sharp or stabbing chest pain during deep breaths, confusion, and an increased respiratory rate.In the elderly, confusion may be the most prominent symptom. The typical symptoms in children under five are fever, cough, and fast or difficult breathing.Fever, however, is not very specific, as it occurs in many other common illnesses, and may be absent in those with severe disease or malnutrition. Additionally, a cough is frequently absent in children less than 2 months old.More severe symptoms may include: central cyanosis, decreased thirst, convulsions, persistent vomiting, or a decreased level of consciousness.
Symptoms frequency in pneumonia
Symptom Frequency
Cough 79–91%
Fatigue 90%
Fever 71–75%
Shortness of breath 67–75%
Sputum 60–65%
Chest pain 39–49%
Cirrhosis is a consequence of chronic liver disease characterized by replacement of liver tissue by fibrosis, scartissue and regenerative nodules (lumps that occur as a result of a process in which damaged tissue is regenerated),leading to loss of liver function. Cirrhosis is most commonly caused by alcoholism, hepatitis B and C, and fatty liver disease, but has many other possible causes. Some cases are idiopathic, i.e., of unknown cause.
Ascites (fluid retention in the abdominal cavity) is the most common complication of cirrhosis, and is associated with a poor quality of life, increased risk of infection, and a poor long-term outcome. Other potentially life-threatening complications are hepatic encephalopathy(confusion and coma) and bleeding from esophageal varices. Cirrhosis is generally irreversible, and treatment usually focuses on preventing progression and complications. In advanced stages of cirrhosis the only option is a liver transplant.
The word "cirrhosis" derives from Greek meaning yellowish, tawny (the orange-yellow colour of the diseased liver) + Eng. med. suff. -osis. While the clinical entity was known before, it was René Laennec who gave it the name "cirrhosis" in his 1819 work in which he also describes the stethoscope.

Encephalitis
Viral Viral encephalitis can occur either as a direct effect of an acute infection, or as one of the sequelae of a latent infection. The most common causes of viral encephalitis are Rabies, Herpies Simplex, Polio, SSPE and PML.Other causes include infection by flaviviruses such as St. Louis encephalitis or West Nile virus, or by Togaviridae such as Eastern equine encephalitis (EEE), Western equine encephalitis (WEE) orVenezuelan equine encephalitis (VEE).
[edit]Bacterial and other
It can be caused by a bacterial infection, such as bacterial meningitis, spreading directly to the brain (primary encephalitis), or may be a complication of a current infectious disease syphilis (secondary encephalitis). Certain parasitic or protozoal infestations, such as toxoplasmosis, malaria, or primary amoebic meningoencephalitis, can also cause encephalitis in people with compromised immune systems. Lyme disease and/or Bartonella henselae may also cause encephalitis.
Another cause is granulomatous amoebic encephalitis.
[edit]Diagnosis
Adult patients with encephalitis present with acute onset of fever, headache, confusion, and sometimes seizures. Younger children or infants may present irritability, poor appetite and fever.
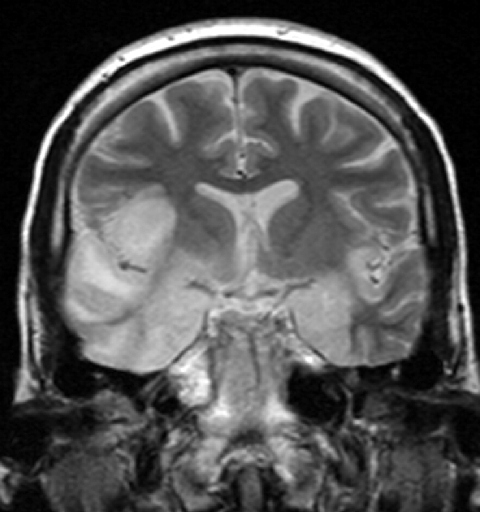
Neurological examinations usually reveal a drowsy or confused patient. Stiff neck, due to the irritation of the meninges covering the brain, indicates that the patient has either meningitis or meningoencephalitis. Examination of the cerebrospinal fluid obtained by a lumbar puncture procedure usually reveals increased amounts of protein and white blood cells with normal glucose, though in a significant percentage of patients, the cerebrospinal fluid may be normal. CT scan often is not helpful, as cerebral abscess is uncommon. Cerebral abscess is more common in patients with meningitis than encephalitis. Bleeding is also uncommon except in patients with herpes simplex type 1 encephalitis. Magnetic resonance imaging offers better resolution. In patients with herpes simplex encephalitis, electroencephalograph may show sharp waves in one or both of the temporal lobes. Lumbar puncture procedure is performed only after the possibility of prominent brain swelling is excluded by a CT scan examination. Diagnosis is often made with detection of antibodies in the cerebrospinal fluid against a specific viral agent (such as herpes simplex virus) or by polymerase chain reaction that amplifies the RNA or DNA of the virus responsible (such as varicella zoster virus).
Treatment
Treatment is usually symptomatic. Reliably tested specific antiviral agents are few in number (e.g. acyclovir for herpes simplex virus) and are used with limited success in treatment of viral infection, with the exception of herpes simplex encephalitis. In patients who are very sick, supportive treatment, such as mechanical ventilation, is equally important. Corticosteroids (e.g. methylprednisolone) are used to reduce brain swelling and inflammation. Sedatives may be needed for irritability or restlessness.
http://en.wikipedia.org/wiki/Encephalitis





Scabies
Scabies (from Latin: scabere, "to scratch"), known colloquially as the seven-year itch, is a contagious skin infection that occurs among humans and other animals. It is caused by a tiny and usually not directly visible parasite, the mite Sarcoptes scabiei, which burrows under the host's skin, causing intense allergic itching. The infection in animals (caused by different but related mite species) is called sarcoptic mange.
The disease may be transmitted from objects but is most often transmitted by direct skin-to-skin contact, with a higher risk with prolonged contact. Initial infections require four to six weeks to become symptomatic. Reinfection, however, may manifest symptoms within as little as 24 hours. Because the symptoms are allergic, their delay in onset is often mirrored by a significant delay in relief after the parasites have been eradicated. Crusted scabies, formerly known as Norwegian scabies, is a more severe form of the infection often associated with immunosuppression.
The disease can be effectively treated with a number of medications. Permethrin cream is the most effective, but expensive compared to other treatments.Crotamiton is less effective, but also nontoxic and soothing. Ivermectin may be used orally and topically. Treatment with lindane preparations has fallen out of favor due to high toxicity and parasite resistance. In order to prevent re-infection, the host's contacts are also often treated
Signs and symptoms
The characteristic symptoms of a scabies infection include intense itching and superficial burrows. The burrow tracks are often linear, to the point that a neat "line" of four or more closely placed and equally developed mosquito-like "bites," is almost diagnostic of the disease.
Pathophysiology
The symptoms are caused by an allergic reaction of the host's body to mite proteins, though exactly which proteins remains a topic of study. The mite proteins are also present from the gut, in mite feces, which are deposited under the skin. The allergic reaction is both of the delayed (cell-mediated) and immediate (antibody-mediated) type, and involves IgE (antibodies, it is presumed, mediate the very rapid symptoms on re-infection). The allergy-type symptoms (itching) continue for some days, and even several weeks, after all mites are killed. New lesions may appear for a few days after mites are eradicated. Nodular lesions from scabies may continue to be symptomatic for weeks after the mites have been killed.


Peptic ulcer
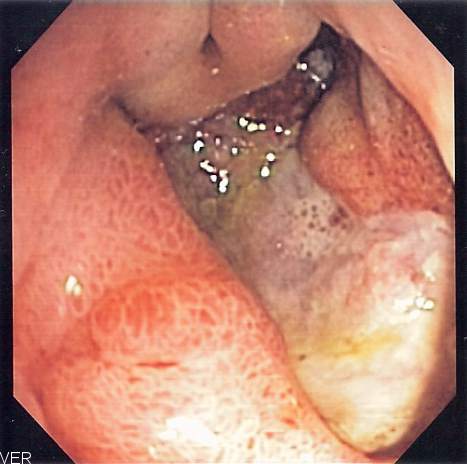
A peptic ulcer, also known as PUD or peptic ulcer disease, the most common ulcer of an area of the gastrointestinal tract that is usually acidic and thus extremely painful. It is defined as mucosal erosions equal to or greater than 0.5 cm. As many as 70–90% of such ulcers are associated withHelicobacter pylori, a spiral-shaped bacterium that lives in the acidic environment of the stomach; however, only 40% of those cases go to a doctor. Ulcers can also be caused or worsened by drugs such as aspirin, Plavix (clopidogrel), ibuprofen, and other NSAIDs.
Signs and symptoms
- abdominal pain, classically epigastric with severity relating to mealtimes, after around three hours of taking a meal (duodenal ulcers are classically relieved by food, while gastric ulcers are exacerbated by it);
- bloating and abdominal fullness;
- waterbrash (rush of saliva after an episode of regurgitation to dilute the acid in esophagus - although this is more associated with GERD);
- nausea, and copious vomiting;
- loss of appetite and weight loss;
- hematemesis (vomiting of blood); this can occur due to bleeding directly from a gastric ulcer, or from damage to the esophagus from severe/continuing vomiting.
- melena (tarry, foul-smelling feces due to oxidized iron from hemoglobin);
- rarely, an ulcer can lead to a gastric or duodenal perforation, which leads to acute peritonitis. This is extremely painful and requires immediate surgery.
A history of heartburn, gastroesophageal reflux disease (GERD) and use of certain forms of medication can raise the suspicion for peptic ulcer. Medicines associated with peptic ulcer include NSAID (non-steroid anti-inflammatory drugs) that inhibit cyclooxygenase, and most glucocorticoids (e.g. dexamethasone and prednisolone).
In patients over 45 with more than two weeks of the above symptoms, the odds for peptic ulceration are high enough to warrant rapid investigation by EGD (see below).
The timing of the symptoms in relation to the meal may differentiate between gastric and duodenal ulcers: A gastric ulcer would give epigastric pain during the meal, as gastric acid production is increased as food enters the stomach. Symptoms of duodenal ulcers would initially be relieved by a meal, as the pyloric sphincter closes to concentrate the stomach contents, therefore acid is not reaching the duodenum. Duodenal ulcer pain would manifest mostly 2–3 hours after the meal, when the stomach begins to release digested food and acid into the duodenum.
Also, the symptoms of peptic ulcers may vary with the location of the ulcer and the patient's age. Furthermore, typical ulcers tend to heal and recur and as a result the pain may occur for few days and weeks and then wane or disappear. Usually, children and the elderly do not develop any symptoms unless complications have arisen.
Burning or gnawing feeling in the stomach area lasting between 30 minutes and 3 hours commonly accompanies ulcers. This pain can be misinterpreted as hunger, indigestion or heartburn. Pain is usually caused by the ulcer but it may be aggravated by the stomach acid when it comes into contact with the ulcerated area. The pain caused by peptic ulcers can be felt anywhere from the navel up to the sternum, it may last from few minutes to several hours and it may be worse when the stomach is empty. Also, sometimes the pain may flare at night and it can commonly be temporarily relieved by eating foods that buffer stomach acid or by taking anti-acid medication. However, peptic ulcer disease symptoms may be different for every sufferer.
Treatment
Younger patients with ulcer-like symptoms are often treated with antacids or H2 antagonists before EGD is undertaken. Bismuth compounds may actually reduce or even clear organisms though the warning labels of some bismuth subsalicylate products indicate that the product should not be used by someone with an ulcer.
Patients who are taking nonsteroidal anti-inflammatories (NSAIDs) may also be prescribed a prostaglandin analogue (Misoprostol) in order to help prevent peptic ulcers, which may be a side-effect of the NSAIDs.
When H. pylori infection is present, the most effective treatments are combinations of 2 antibiotics (e.g. Clarithromycin, Amoxicillin, Tetracycline, Metronidazole) and 1 proton pump inhibitor (PPI), sometimes together with a bismuth compound. In complicated, treatment-resistant cases, 3 antibiotics (e.g. amoxicillin + clarithromycin + metronidazole) may be used together with a PPI and sometimes with bismuth compound. An effective first-line therapy for uncomplicated cases would be Amoxicillin + Metronidazole + Pantoprazole (a PPI). In the absence of H. pylori, long-term higher dose PPIs are often used.
Treatment of H. pylori usually leads to clearing of infection, relief of symptoms and eventual healing of ulcers. Recurrence of infection can occur and retreatment may be required, if necessary with other antibiotics. Since the widespread use of PPI's in the 1990s, surgical procedures (like "highly selective vagotomy") for uncomplicated peptic ulcers became obsolete.
Perforated peptic ulcer is a surgical emergency and requires surgical repair of the perforation. Most bleeding ulcers require endoscopy urgently to stop bleeding with cautery, injection, or clipping.
Ranitidine provides relief of peptic ulcers, heartburn, indigestion and excess stomach acid and prevention of these symptoms associated with excessive consumption of food and drink. Ranitidine is available over the counter from a pharmacy and works by decreasing the amount of acid the stomach produces allowing healing of ulcers. Zantac tablets contain Ranitidine 150 mg as the active ingredient which can also be bought generically.
Sucralfate, (Carafate) has also been a successful treatment of peptic ulcers.
Colles' fracture
A Colles' fracture, also Colles fracture, is a fracture of the distal radius in the forearm with dorsal (posterior) displacement of the wrist and hand. The fracture is sometimes referred to as a "dinner fork" or "bayonet" deformity due to the shape of the resultant forearm. For a more detailed discussion seedistal radius fracture.
Causes
The fracture is most commonly caused by people falling onto a hard surface and breaking their fall with outstretched arms - falling with wrists flexed would lead to a Smith's fracture. It can also be caused by overuse. Orignally it was described in elderly people, post-menopausal women. It usually occurs about an inch or two proximal to the radio-carpal joint with posterior and lateral displacement of the distal fragment resulting in the characteristic "dinner fork" or "bayonet" like deformity.Colles' fracture is a common fracture in people with osteoporosis, second only to vertebral fractures.
Treatment
Management depends on the severity of the fracture. An undisplaced fracture may be treated with a cast alone.The cast is applied with the distal fragment inpalmar flexion and ulnar deviation. A fracture with mild angulation and displacement may require closed reduction. There is some evidence that immobilization with the wrist in dorsiflexion as opposed to palmarflexion results in less redisplacement and better functional status. Significant angulation and deformity may require an open reduction and internal fixation or external fixation. The volar forearm splint is best for temporary immobilization of forearm, wrist and hand fractures, including Colles' fracture There are several established instability criteria: dorsal tilt >20°, comminuted fracture, abruption of the ulnar styloid process, intraarticular displacement >1mm, loss of radial height >2mm.A higher amount of instability criteria increases the likelihood of operative treatment.Treatment modalities differ in the elderly.

Myxedema
Myxedema (British English: myxoedema) describes a specific form of cutaneous and dermal edema secondary to increased deposition of connective tissuecomponents (like glycosaminoglycans, hyaluronic acid, and other mucopolysaccharides) in subcutaneous tissue as seen in various forms of hypothyroidismand Graves' disease.]:535 It is more common in women than in men.
Cause
The increased deposition of glycosaminoglycan is not fully understood, however two mechanisms predominate.
- Exophthalmos in particular results from TSH receptor stimulation on fibroblasts behind the eyes which leads to increased glycosaminoglycan deposition. It is thought that many cells responsible for forming connective tissue react to increases in TSH levels.
- Secondarily, in autoimmune thyroid diseases lymphocytes react to the TSH receptor. Thus, in addition to the inflammation within the thyroid, any cell that expresses the TSH receptor will likely experience lymphocytic infiltrates as well. The inflammation can cause tissue damage and scar tissue formation, explaining the deposition of glycosaminoglycans.The increased deposition of glycosaminoglycans causes an osmotic edema and fluid collection.Hashimoto's thyroiditis is the most common cause of myxedema in the United States.
Symptoms
Symptoms of myxedema include thickening of the skin and other symptoms associated with hypothyroidism, including fatigue, weight gain, Depression, dry skin, and brittle hair, among others. Skin thickening or swelling associated with myxedema is often described as nonpitting edema. In other words, if you press on the skin of the affected area and then remove your finger, you will not see an imprint.
TREATMENTS
Myxedema is most often addressed by treating the underlying cause of hypothyroidism that led to the thickening and coarseness of the skin. Medication to replace the reduced thyroid hormones is the most common treatment, and when dosed appropriately, may halt the progression of myxedem

สมัครสมาชิก:
บทความ (Atom)

